S. Ahmad
World TB Day is commemorated on March 24 to raise public awareness about the devastating health, social and economic consequences of TB. It reminds us to step up efforts to end the global TB epidemic. The date commemorates 1882, when Dr. Robert Koch announced his discovery of Mycobacterium tuberculosis, the bacterium that causes TB, opening the door to diagnosis and cure. Yet more than a century later, tuberculosis remains one of humanity’s deadliest infectious diseases. For India, which has long carried the world’s highest TB burden, the day is not symbolic—it is strategic. It is a measure of how far the country has come, and how far it must still go.
The encouraging news is this: India is no longer merely fighting tuberculosis; it is actively dismantling it. According to the World Health Organization’s Global Tuberculosis Report 2025, new TB cases in India declined by 21 percent between 2015 and 2024—one of the sharpest drops among high-burden nations. During the same period, TB-related deaths fell by 28 percent. These are not incremental shifts; they represent a structural transformation in detection, treatment, and community engagement.
Behind these numbers lies a deliberate and multi-layered public health response. India has set itself an ambitious target—to eliminate tuberculosis by 2025, five years ahead of the global Sustainable Development Goal timeline. Skeptics initially viewed the deadline as aspirational. Today, it looks increasingly attainable.
Tuberculosis is caused by the bacterium Mycobacterium tuberculosis and most commonly affects the lungs, though it can also damage the brain, kidneys, and spine. Not everyone infected becomes sick. Some individuals carry latent TB infection without symptoms or the ability to transmit the disease. However, when TB becomes active, it spreads through the air—via droplets released when an infected person coughs, sneezes, or speaks, particularly in poorly ventilated spaces. Contrary to persistent myths, TB does not spread through handshakes, shared meals, or casual contact. Importantly, patients with pulmonary TB typically stop being infectious after two weeks of proper treatment.
Understanding the disease is critical because TB is both medical and social. It thrives where poverty, malnutrition, overcrowding, and limited healthcare access persist. Eliminating TB, therefore, requires more than medicines; it requires systemic reform.
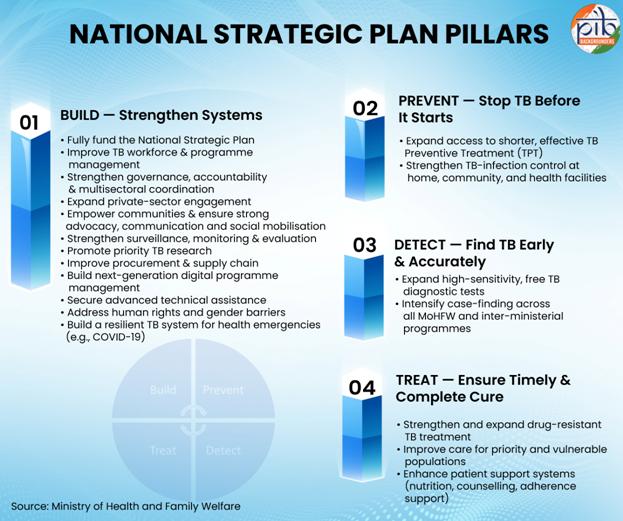
India’s response is anchored in the National Strategic Plan (2020–25), built on four pillars: Detect, Treat, Prevent, and Build. This framework reflects a shift from passive case detection to proactive outreach, from episodic treatment to patient-centric support, and from fragmented efforts to a whole-of-government and whole-of-society approach.
In 2020, the government renamed the Revised National Tuberculosis Control Programme as the National TB Elimination Programme (NTEP), signaling not just continuity but acceleration. The rebranding underscored a new urgency: India would not merely control TB—it would end it.
Early diagnosis has become central to this mission. The country now operates more than 9,800 rapid molecular testing facilities and 107 culture and drug-susceptibility laboratories—the largest such diagnostic network in the world. These facilities enable faster and more accurate identification of TB and drug-resistant strains, reducing delays that once fueled transmission.
But diagnosis alone does not cure. Treatment adherence has historically been one of the biggest challenges in TB control. Standard TB therapy lasts at least six months, and longer for drug-resistant cases. Interruptions can lead to relapse and resistance.
To address this, the government launched the Pradhan Mantri TB Mukt Bharat Abhiyaan in September 2022, transforming TB elimination into a Jan Andolan—a people’s movement. The campaign seeks to mobilize communities, corporate social responsibility initiatives, and local governance structures to support patients beyond clinical care.
Nutrition plays a critical role in recovery. TB patients often experience weight loss and weakness, and treatment drugs can exacerbate side effects if dietary intake is poor. Under the Nikshay Poshan Yojana, launched in 2018, every notified TB patient receives ₹1,000 per month as nutritional support. Since its inception, over ₹4,454 crore has been directly transferred into the bank accounts of 1.38 crore beneficiaries. This is not charity; it is public health economics—reducing treatment default and improving recovery rates.
Complementing financial support is the Ni-kshay Mitra initiative, which invites individuals, NGOs, corporations, religious groups, and volunteers to adopt TB patients. These “TB Friends” provide food baskets, psychosocial encouragement, and sometimes vocational guidance. As of November 2025, more than 6.77 lakh Ni-kshay Mitras had distributed over 45 lakh food baskets. The participation of over two lakh My Bharat youth volunteers illustrates how public health can unify generations in shared purpose.
The most intensive recent push came through the 100-Day TB Mukt Bharat Abhiyan, launched on December 7, 2024, across 347 high-priority districts. Through vulnerability mapping and systematic screening, more than 20 crore individuals from high-risk populations were screened. Over 28 lakh TB patients were diagnosed, including nearly 9 lakh asymptomatic cases that might otherwise have remained hidden reservoirs of transmission.
The results have been striking. Treatment success rates under the expanded campaign have climbed to 90 percent—surpassing the global average of 88 percent. Over 46,118 Gram Panchayats were certified TB-free in 2024, reflecting not just administrative achievement but community ownership.
Innovation has further strengthened India’s strategy. Drug-resistant TB, once considered one of the most formidable obstacles to elimination, is being tackled with the introduction of the BPaLM regimen—a shorter, safer, and highly effective combination therapy including Bedaquiline, Pretomanid, Linezolid, and Moxifloxacin. This six-month course replaces longer, more toxic regimens of the past. More than 15,000 MDR/RR-TB patients have already been initiated on this treatment, offering renewed hope against resistance.
Prevention, too, has gained prominence. TB Preventive Treatment (TPT) is now administered to eligible household contacts, children, and people living with HIV, preventing latent infections from progressing to active disease. By integrating preventive therapy with active case-finding campaigns, India is targeting transmission at its roots.
Technology has become an unexpected ally. India’s TB programme is increasingly AI-driven. The “Cough Against TB” initiative uses acoustic artificial intelligence to analyze a three-second smartphone recording of a cough for TB signatures, reportedly increasing case detection yields by 12–16 percent. Radiology AI platforms such as DeepCXR assist in interpreting chest X-rays, particularly in regions lacking specialist radiologists. Predictive analytics systems flag patients at high risk of adverse outcomes, contributing to a reported 27 percent reduction in treatment failures following nationwide deployment.
These tools are not replacing doctors; they are amplifying reach, particularly in rural and underserved regions.
Consider the example of Gurez Valley in Bandipora district of Kashmir—an isolated Himalayan region cut off during winter. There, mobile vans equipped with portable X-ray machines and diagnostic tools screened 1,250 residents over three days, identifying more than 250 potential TB cases. Health teams collaborated with local leaders and even the Indian Army to conduct awareness sessions. This is what elimination looks like on the ground: technology meeting terrain, science meeting society.
Healthcare infrastructure has also expanded through Ayushman Arogya Mandirs under the broader Ayushman Bharat scheme. As of March 2026, 1,84,726 such centers operate across India, providing accessible primary care. These centers act as first points of contact for individuals with TB symptoms, ensuring early diagnosis and referral.
The cumulative effect of these interventions is visible in the national trendline. A 21 percent decline in incidence and a 28 percent reduction in mortality over nine years signal that policy, when sustained and inclusive, can bend the curve of disease.
Yet challenges remain. Urban overcrowding, migrant populations, diabetes co-morbidity, and antimicrobial resistance continue to complicate progress. Stigma still discourages some individuals from seeking timely diagnosis. Funding must remain consistent, and surveillance systems vigilant, even as numbers decline.
Public health victories are fragile if complacency sets in.
The larger lesson from India’s TB trajectory is that elimination is not a singular event but a process—one that integrates science, governance, social protection, and community empathy. It demands data-driven strategy and human-centered compassion.
India’s sprint towards TB elimination is therefore more than a domestic achievement; it is a global case study. It demonstrates that high-burden countries can accelerate progress through political will, technological adoption, and grassroots mobilization. It shows that eliminating an airborne infectious disease in a population of over 1.4 billion is not utopian—it is operational.
World Tuberculosis Day serves as both reminder and resolve. The discovery of the TB bacterium in 1882 opened the door to cure. India’s present campaign is opening the door to eradication.
If current momentum continues—if communities stay engaged, if innovation keeps pace, and if vigilance remains uncompromised—the vision of a TB-free India by 2025 may shift from ambition to reality.
In the story of global health, tuberculosis has long been a chapter of loss. India is attempting to rewrite it as a chapter of determination.
Comments are closed.